
Hip osteotomies are used to cut the bone and redirect the fragments to improve the joint function. All hip osteotomies can cause interruption to the blood supply to the ball and induce cartilage damage in the hip.
Femoral Osteotomies
Femoral osteotomies are used to redirect the ball into the socket. The cuts are usually made at the site of the abnormality. Deformities of the head and neck are treated with osteotomies made either directly at the site of abnormality or farther away creating a compensatory deformity to balance the hip condition. The farther osteotomies are considered safer. The osteotomies are usually fixed with plates and screws. A body cast may also be used in very young children. They take 6 to 12 weeks to heal and the metallic implants are usually removed within 6 to 12 months.





Acetabular Osteotomies
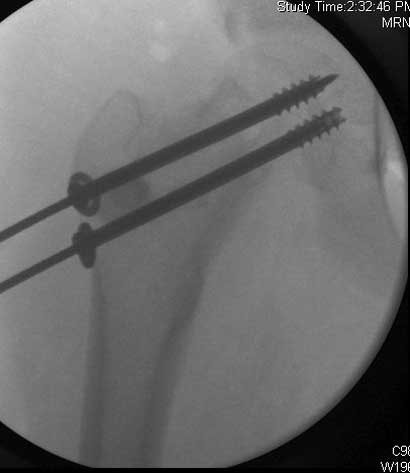
Acetabular osteotomies are used to deepen a shallow socket, redirect the socket, or rarely correct a very deep socket. These surgeries can cause significant blood loss especially with the more complex surgeries in the older children. Metal pins, or screws are occasionally used. In young children body casts are used for 6 weeks and the metal implants are removed early.
Figure E1

Periacetabular Osteotomy
Considered to be the best for treating a shallow socket in skeletally mature children. Performed by a select few surgeons due to the technical difficulty.
A single incision in the front of the socket allows disconnection of the socket from the reminder of the pelvis allowing repositioning of the socket in a more desirable position. Has several advantages over similar osteotomies. Blood loss can be decreased by multiple techniques including collecting the blood from the wound and transfusing it back to the patient. The ideal position of the socket may not be achieved during the first operation and it may be desirable to reposition the socket early as a simpler second procedure.
Preventive measures will be taken to avoid infections, blood clots, and blood transfusions routinely but complications cannot be prevented completely.
Figure D1
Figure D2