
Hip dysplasia commonly refers to acetabular dysplasia — particularly acetabular deficiency in covering the femoral head. Deficiency can be global or focal to lateral coverage by the sourcil, or anterior or posterior wall coverage. Instability suggests a hip's tendency to subluxate or dislocate. Acetabular dysplasia alone or in combination with proximal femoral morphology facilitates hip instability.
Risk factors for lateral instability include acetabular under-coverage laterally, an upsloping sourcil, and coxa valga. Additional anterior deficiency combined with femoral anteversion causes anterosuperior instability; posterior acetabular deficiency with femoral retroversion causes posterosuperior instability. Conversely, coxa vara can compensate for lateral dysplasia, and femoral version in the opposite direction can compensate for acetabular wall deficiency.

Chronic progressive hip instability commonly occurs with simple weight bearing, inducing lateral subluxation of the head. This is resisted initially by hypertrophy of the labrum, capsule, ligamentum teres, and muscles. Subluxation becomes symptomatic in older children when the hypertrophied labrum degenerates and tears. These labral tears are unique inside-out avulsions that can tear articular cartilage and acetabular rim bone — the fractured lateral rim is called a rim fracture or os acetabuli. Edge loading on the lateral acetabulum produces degeneration of both the femoral head and acetabular cartilage, known as acetabular rim syndrome.
Clinical Features
Dysplasia in children is usually not painful. A limp and limb shortening can be seen with subluxation or dislocation. Pain after prolonged standing and walking is usually from abductor fatigue. Hip range of motion is increased, especially FIR, with a positive anterior impingement sign. Apprehension sign is positive for anterior and posterior instability.
Imaging
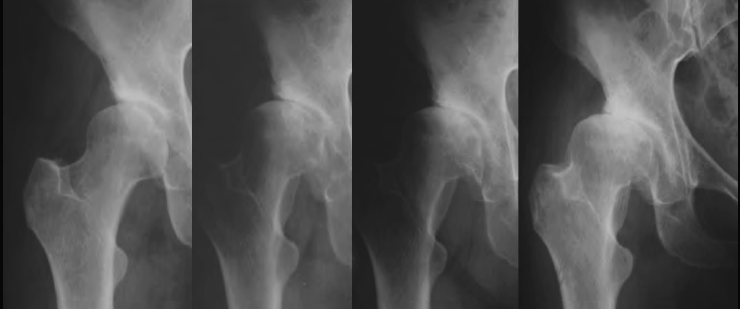
Lateral subluxation is seen on AP view as a break in Shenton's line, decreased LCE, narrowed lateral joint space, and widened medial space. Anterior subluxation is seen on the faux profil view as decreased ACE, narrowed anterior joint space, and posterior space widening. Reducibility of the femoral head can be confirmed with an abduction-internal rotation X-ray (AIR view). CT can show femoral head and acetabular shape well. MRI can show labral tear, hypertrophy, labral cysts, and cartilage damage.
Treatment
Subluxation is a sign of instability, poor prognosis, and a strong indication to intervene at any age. Dysplasia in young children can be treated with abduction bracing or femoral osteotomy, expecting acetabular remodelling. After age 4, acetabular remodelling does not reliably correct dysplasia and acetabular osteotomy is ideal. Femoral varus osteotomy can compensate for mild acetabular dysplasia but causes shortening, abductor weakness, and lateral hip prominence. Severe varus (<100°) stops compensating for dysplasia and starts contributing to lateral subluxation.
Indications for Additional Femoral Osteotomy
- High subluxation and soft tissue tension requiring femoral shortening to reduce the head and rotate the acetabulum
- Inadequate acetabular correction
- Persistent foveal contact with the sourcil
- Irreducible femoral head (aspherical or too large)
- Valgus osteotomy to match a flat head to a flat sourcil
Goal of Reconstruction
Good hip reconstruction aims to reduce a round femoral head deep into a flat acetabulum with good anterior and posterior wall coverage. This may require femoral shortening, varus or valgus osteotomy, open reduction, cam osteoplasty, and head reduction osteotomy as needed.
Once the head is placed well, the acetabulum needs modification to prevent subluxation: bending the acetabular roof (Pemberton, Dega) if enlarged and steep; redirecting the acetabulum (Salter, Triple, PAO) without changing its shape; or enlarging the acetabulum with bone support over the capsule (Chiari, shelf) when the head is not reducible or the acetabulum is already flat. For poor acetabular development, capsular interposition arthroplasty (tectoplasty or Colonna arthroplasty) may be required. If the head is absent or too small, trochanteric arthroplasty or valgus osteotomy for pelvic support are options. Advanced cartilage damage can be treated with arthrodesis, excision arthroplasty, or total hip arthroplasty.

Medial Dysplasia
Medial dysplasia is a rare entity of medial deficiency of the head by a short sourcil, causing medial arthritis from foveal impingement rather than true instability. Medial coverage is measured with the medial center-edge angle (MCE), ideally ≥20°. When medial dysplasia is coupled with a negative sourcil angle, there is medial subluxatory stress on the femoral head and increased weight bearing on the acetabular fossa, loading the fovea and crushing the ligamentum teres.
Medial dysplasia can be combined with lateral over-coverage and impingement. This combination requires a reverse acetabular osteotomy — rim trimming alone would make the total sourcil width too small. Medial rotation of the PAO to flatten the sourcil lateralises the inferior acetabulum and decreases adduction and rotations in extension from impingement, so the inferior parts of both walls need to be resected. This correction also requires pubic shortening and femoral nerve decompression.
Posterosuperior Dysplasia
The posterior wall may cross close to the centre of the head yet still be deficient superiorly. Posterior wall LCE measured to the point where it touches the sourcil of less than 20° is an indication to consider an anteverting PAO in a young patient who will not yet have anterolateral arthritis.
Lateral Dysplasia
LCE is only one measure of lateral coverage. Consider all three sourcil parameters together — total size (LCE + MCE, or a total arc of 50–60°), concavity of shape, and sourcil angle. The sourcil angle is the most important parameter: ideally flat or perpendicular to the primary compression trabeculae. With these measures, the aim is to determine whether the sourcil will allow lateral subluxation, rim loading, labral tear, and eventual arthritis.