Pelvis
The human pelvis is a bony ring made of the sacrum posteriorly and two innominate bones on the sides and anteriorly. There is no inherent bony stability — the three bones are held together by the strong sacroiliac ligaments posteriorly, the sacrospinous and sacrotuberous ligaments in the pelvic floor, and the pubic symphysis anteriorly. These structures bear more load during daily activities than their intrinsic strength can withstand, suggesting that dynamic muscle forces protect them from injury during high-intensity activities.
Each innominate bone is formed by fusion of the ilium, pubis, and ischium at the triradiate cartilage in the acetabulum. Damage to the triradiate cartilage before age 8 can cause post-traumatic dysplasia, characterised by a steep sourcil, wide V-shaped teardrop, thick iliac part of the acetabulum, and relative retroversion (more posterior than anterior dysplasia with a crossover sign). Triradiate cartilage fusion has been discussed as a treatment option for protrusio acetabuli in children. The limbus (unossified lateral acetabulum and labrum complex) contributes approximately 30% of acetabular depth.
Posterior Wall Development
The posterior wall is not fully ossified until triradiate cartilage closure. Apparent posterior wall deficiency (false crossover sign) is seen on X-rays in 90% of girls under 12 and boys under 14. Posterior wall fractures can be missed or underestimated on X-rays and CT — MRI is recommended after post-traumatic hip dislocations in children.
Femoral Head & Acetabulum — Mutual Influence
The shape of the head determines the shape of the acetabulum and vice versa. An aspherical head — as in Perthes, SCFE, and idiopathic cam with open triradiate cartilage — makes the acetabulum wide anteriorly and laterally, allowing the cam to enter farther. This is seen as lateral joint space widening.
Conversely, a shallow acetabulum leaves the head aspherical with cam morphology, while a deep acetabulum causes the head to be very round with a narrow neck. Cam morphology is commonly seen with acetabular dysplasia, likely from inadequate rounding of the head because the socket was not deep enough to influence head shape. Protrusio hips have a very spherical head with a narrow neck (low alpha angle). The combination of protrusio and cam is less common but very likely to become symptomatic early.
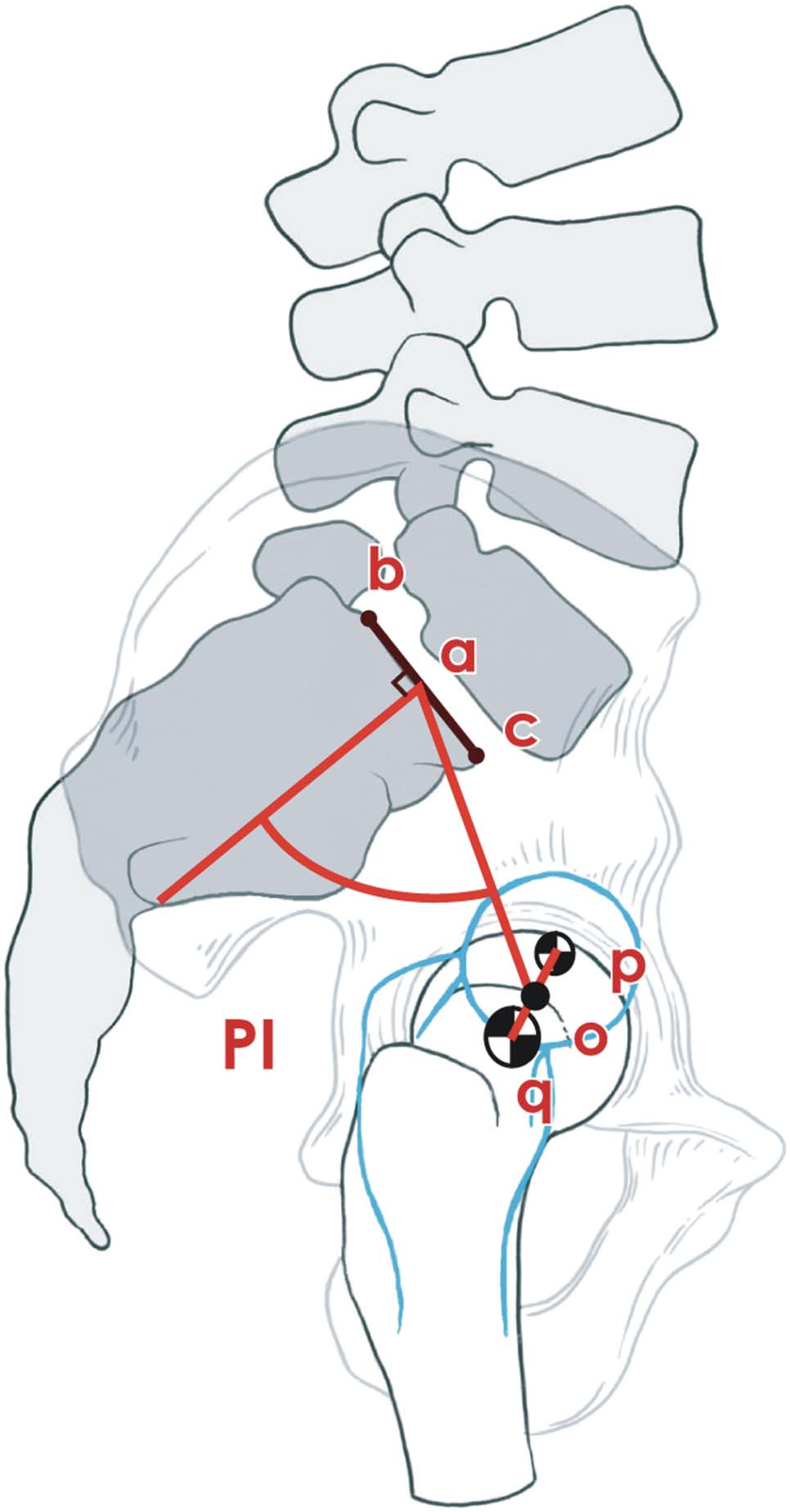
Pelvic Incidence
The fixed structural relationship of the acetabulum to the sacrum is measured on the lateral view by the angle subtended between the line perpendicular to the S1 end plate and another line connecting the centres of the S1 end plate and the femoral head. Pelvic incidence (PI) is determined at birth and changes slightly during development. PI determines the position of the hips, pelvic tilt, shape of the buttocks, and spinal alignment. An anterior opening wedge innominate osteotomy can theoretically decrease PI; a closing wedge osteotomy can increase it.
Acetabulum
The acetabulum is an incomplete cup in the innominate bone. The articular cartilage is inverted U-shaped, distributed anteriorly, posteriorly, and superiorly around the acetabular fossa. The acetabulum covers approximately 70% of the femoral head. The acetabular fossa itself does not articulate with the femoral head. A high fossa decreases the medial extension of the articular cartilage in the dome and reduces medial coverage of the femoral head.
The reflected head of the rectus femoris inserts at the top of the acetabulum (12 o'clock position). The iliopsoas tendon crosses the anterior wall at the mid-anterior part (3 o'clock for the right hip). The acetabular wall is thin at 12 o'clock, thickens toward the AIIS, and becomes thin again at 3 o'clock — this triangular morphology allows anterior rim trimming in the correct location without intraoperative fluoroscopy. The middle of the transverse acetabular ligament is at 6 o'clock.
The anterior half of the acetabulum, together with the iliac crest and superior pubic ramus, forms the anterior column. The posterior half, together with the ilium extending to the SI joint and the ischium, forms the posterior column. The thin medial wall is called the quadrilateral plate.
Acetabular Labrum
The labrum is a fibrocartilaginous extension of the articular cartilage at the periphery. A cleft between the articular cartilage and labrum is normal posteriorly, but the labrum and cartilage are continuous anteriorly — any disruption of the anterior chondrolabral junction is pathological. The labrum increases acetabular depth and forms a suction seal around the head, continuing inferiorly as the transverse acetabular ligament. A recess adjacent to the transverse acetabular ligament allows branches of the obturator nerve and artery to enter the hip.
The ligamentum teres originates from the transverse acetabular ligament and inserts into the fovea centralis. The labrum is separated from the hip capsule by a recess, so capsular stresses are not normally transmitted to the labrum — this recess fills with scar in inflammation. The labrum has blood supply only on its outer aspect but heals well when repaired or reconstructed.
Muscles 27 muscles cross the hip
| Muscle | Function & Clinical Notes |
|---|---|
| Gluteus medius | Primary abductor; weakness causes lateral lurch and increases shear forces on acetabular cartilage during walking |
| Gluteus maximus & hamstrings | Extend the hip; weakness increases anterior pelvic tilt |
| Iliopsoas | Primary hip flexor; can stabilise the hip anteriorly |
| Gluteus minimus | Primary internal rotator; attached to the hip capsule |
| Hip adductors | Stabilise the hip in co-contraction with other muscle groups |
Nerves
| Nerve | Course & Clinical Significance |
|---|---|
| Superior gluteal nerve | Supplies hip abductors and internal rotators; at risk from traction injury during posterior and lateral approaches as it passes anteriorly between gluteus medius and minimus, coursing 3–4 cm above the greater trochanter |
| Femoral nerve | Courses on the anteromedial aspect of iliopsoas in the femoral triangle |
| Sciatic nerve | Crosses the short external rotators posteriorly; always superficial to quadratus femoris |
| Obturator nerve | Innervates the medial hip; thought to cause referred pain from the hip to the knee |
| Lateral femoral cutaneous nerve (LFCN) | Emerges from under the inguinal ligament near the ASIS; the most commonly injured nerve during anterior approaches and anterior arthroscopic portals |
Blood Supply to the Hip Joint
- Lateral circumflex femoral artery — supplies the anterior hip capsule and femoral neck; does not contribute directly to femoral head blood supply
- Obturator artery — supplies the medial capsule, acetabulum, ligamentum teres, and a small portion of the head around the fovea centralis; not clinically significant to the head
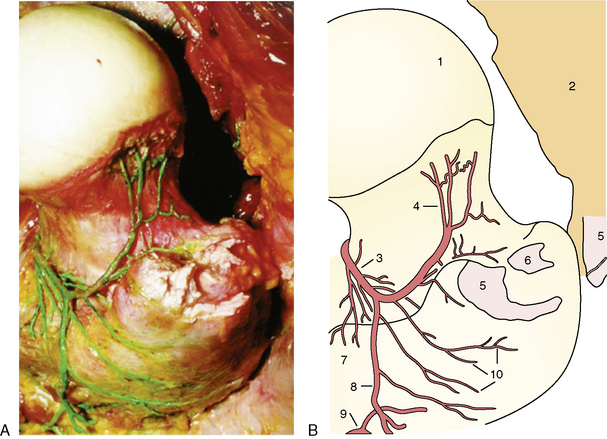
- Medial circumflex femoral artery — the critical supply to the femoral head. Arises in the femoral triangle from the profunda femoris or femoral artery, travels posteriorly over iliopsoas along the inferior border of obturator externus. Its deep branch gives rise to medial retinacular vessels that travel along the posterior aspect of the medial synovial fold (ligament of Weitbrecht) to supply the inferior femoral head. Its ascending branch receives blood from the piriformis branch of the inferior gluteal artery before crossing the obturator externus tendon, entering the hip capsule, and coursing up the neck in the lateral synovial fold. The lateral retinacular artery divides into 2–5 branches as they enter the femoral head at the articular cartilage border. These vessels can nourish the entire femoral head independently when all other blood supply is interrupted. Disruption of these vessels cannot be acutely compensated by any other supply. After physeal closure, metaphyseal vessels may supply the head in some hips. No other significant anastomosis contributes to femoral head blood supply.
The acetabulum is supplied by the superior gluteal artery laterally, iliolumbar artery from the inner table, and obturator artery inferomedially — adequate flow is possible from any one of these sources.