Femoral head fractures are usually associated with hip dislocation. They can involve both the non-weight-bearing portion of the head (Pipkin 1) and the weight-bearing dome (Pipkin 2). Though a small inferior head fracture does not bear much load, it must contribute to hip stability if the piece broke during dislocation. The textbook answer is non-operative treatment if the fragment is close to its defect and does not block motion. Dr. Prasad Gourineni tends to fix them all through an anterior approach. One was fixed arthroscopically with some difficulty because the guide wires and depth gauges for the 3.0 headless screws were not long enough. More complex or comminuted fractures and posterior wall fractures can be accessed with the surgical dislocation approach.
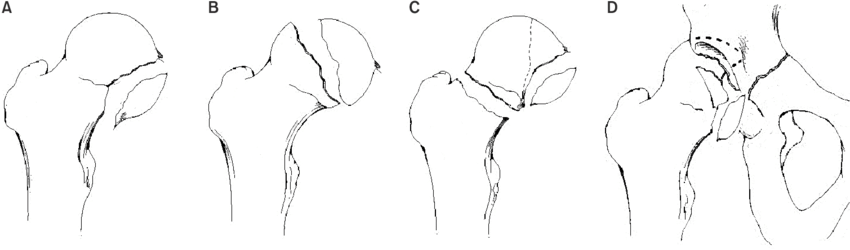
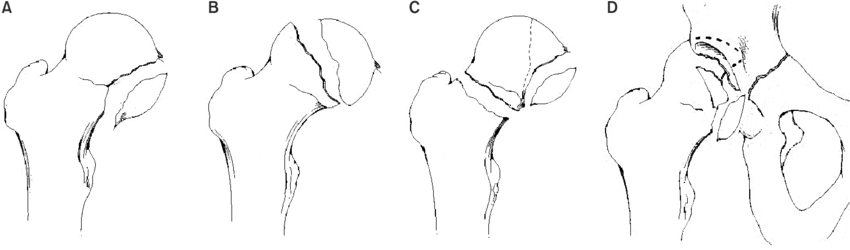
Pipkin Classification
| Type | Description |
|---|---|
| A (Pipkin 1) | Inferior fragment |
| B (Pipkin 2) | Dome fragment |
| C (Pipkin 3) | Associated femoral neck fracture |
| D (Pipkin 4) | Associated acetabular fracture |
Open Technique
The Smith-Petersen approach going medial to rectus is usually adequate to reduce and fix most head and neck fractures. Drill hole assessment of femoral head vascularity is useful to rule out AVN.
Arthroscopic Technique
Once the initial blood is cleared from the joint with high flow and epinephrine in saline, pressures can be lowered to 40–50 mmHg. Swelling occurs very often but rarely causes any problems. Reduction of the fracture is achieved by direct manipulation of the fragment into its defect in the head, with the acetabulum acting as a template. For screw fixation, the guide wire can be placed percutaneously and whenever the angle is right a small incision is made for drilling and screw placement. The portals can be placed anywhere lateral to the ASIS and sciatic nerve.