Standard Anterior Approach (Smith-Petersen)
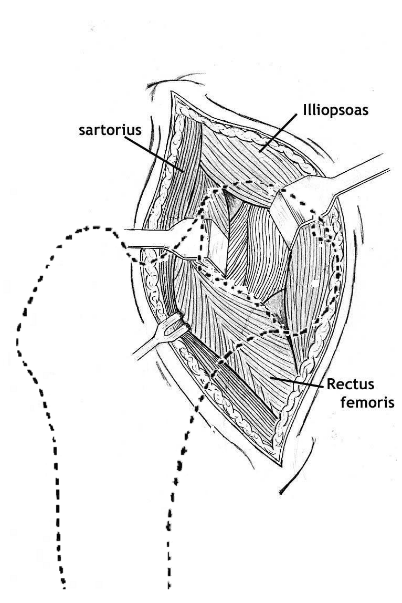
The straight anterior approach (Smith-Petersen) is the most common open approach used. The standard interval is between the sartorius and tensor fascia lata (TFL) superficially, and between the rectus femoris (RF) and gluteus medius deeply. A deeper interval — not commonly described — lies between the iliocapsularis (IC) anteriorly and gluteus minimus posteriorly. Both muscles are attached to the capsule and require elevation of their red fibres off the white capsule. Branches of the lateral femoral circumflex artery and other minor named vessels are encountered and cauterised without difficulty.
Incising the fascia over TFL lateral to the TFL-sartorius interval and retracting all TFL fibres laterally protects the main branch of the lateral femoral cutaneous nerve (LFCN) without even exposing it. More medial exposure of the joint, anterior wall, and superior pubic ramus requires release of the RF origin and retraction medially, or working medial to RF by retracting it laterally. The nerve supply to the rectus from the femoral nerve limits lateral retraction and distal extension of this interval.
Indications
The anterior approach is useful for the following procedures:

Technique
Anterior Approach Medial to Rectus Femoris
The standard anterior approach does not expose the hip joint adequately without release or relaxation of the rectus femoris tendon. Dr. Prasad Gourineni uses a less invasive anterior approach medial to the rectus tendon for the following procedures:
- Draining septic hips
- Acetabular rim trimming
- Labral repair
- Femoral neck osteoplasty
- Open reduction of femoral head and neck fractures
The safety of this approach was confirmed in cadavers — the proximal branch innervating the rectus tendon was consistently distal to the hip joint (unpublished data).