Femoral neck fractures, when displaced in physiologically young people, are best treated with anatomic reduction and screw fixation promptly. Elderly patients are better treated with replacement of the femoral head. Results are better with open reduction through the Smith-Petersen approach going medial to rectus femoris. With open reduction, the haemarthrosis can be decompressed well, fracture reduction can be improved, and femoral head vascularity evaluated by drilling a small hole in the head and looking for active bleeding.
Technique
Manipulate the head with a joystick, traction, and internal rotation of the neck. Aim for anatomic or slight valgus reduction. A clamp can be used to compress the fracture site. Internal fixation with 2–3 screws is standard. DHS has been shown to be stronger but carries a higher AVN rate. In adults, 3 screws are standard.
Dr. Gourineni's Technique
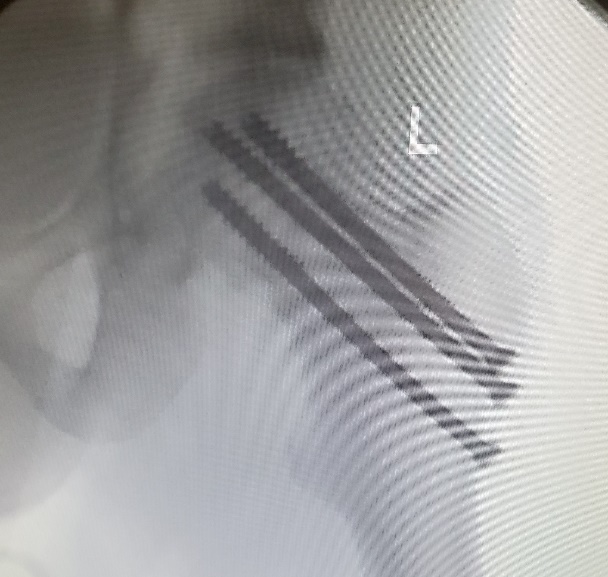
Uses two short-threaded screws to lag the head into slight valgus and places a fully threaded screw along the calcar to prevent shortening. All screws start laterally above the level of the lesser trochanter, are placed juxtacortical in the neck, and advanced close to the subchondral bone. In older children the physis can be ignored and crossed with the screws; in younger children, screws can end short of the physis and guide wires can be left in the head to protect the epiphysis from slipping.
Biplane Double Support Fixation (BDSF) with screws has been supported by two large series in older patients.