Avulsion of bone fragments is not uncommon in children with open cartilage at sites of tendon attachment. There are multiple sites around the hip that sustain these injuries, and they are more commonly associated with stiff hips and hip impingement. Muscles are tighter on the side of hip impingement. The need for surgical treatment for fractures displaced more than 10 mm is controversial.
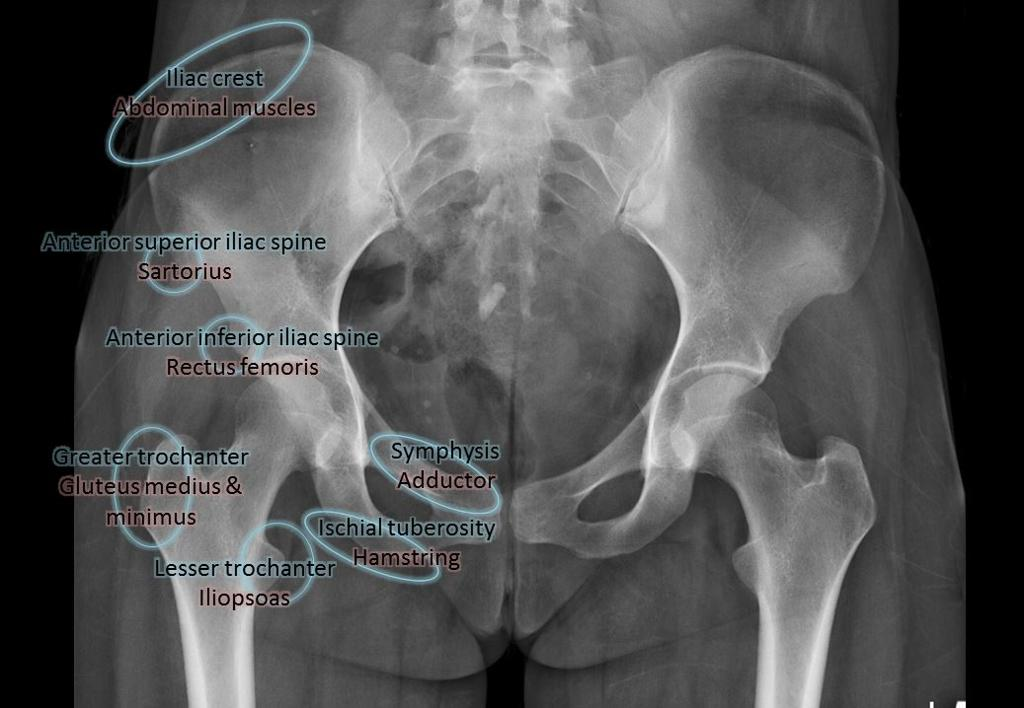
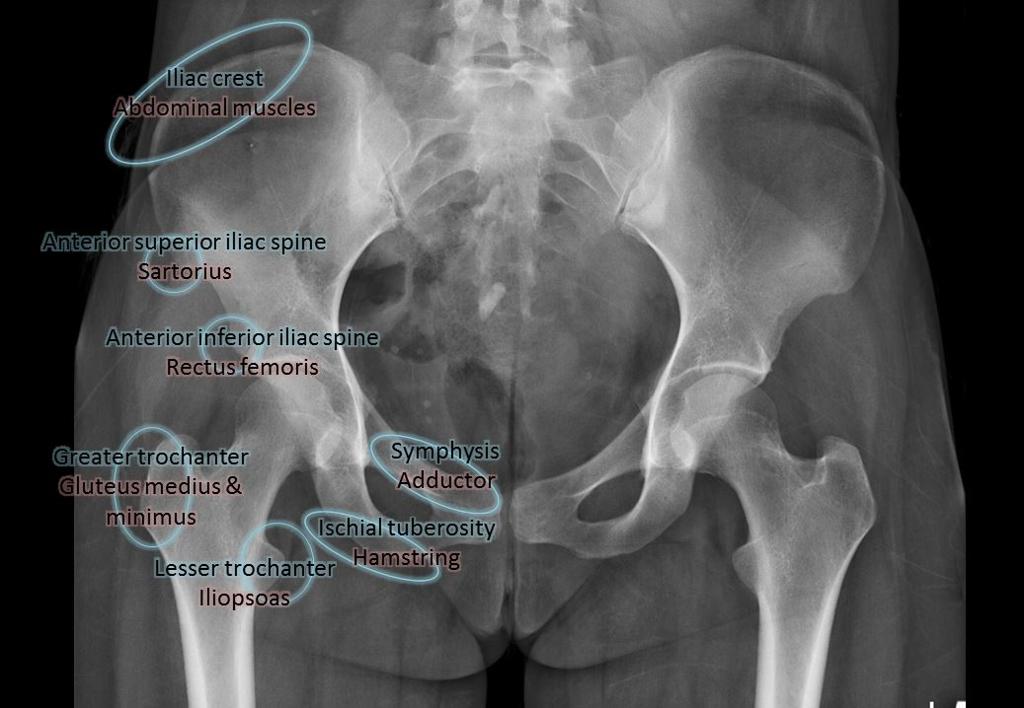
Avulsion Fracture Sites
| Site | Muscle / Cause | Notes |
|---|---|---|
| AIIS | Straight head of rectus femoris; soccer/football | Heals quickly; can leave bony prominence causing subspine impingement. No indication for acute repair. |
| ASIS | Sartorius; forced flexion | Pain resolves quickly; resume activities as tolerated. |
| Iliac crest | Abdominal muscles | Heals well with early mobilisation. |
| Pubic tubercle | Adductor longus and pectineus | Heals well with activity modification. |
| Pubic symphysis | Rectus abdominis | Usually treated non-operatively with early mobilisation. |
| Ischial tuberosity | Proximal hamstring tendons | Complete ruptures cause chronic pain and weakness. Surgical repair has better outcomes but more complications. |
| Greater trochanter | Direct trauma; hip abductors | High risk of AVN in children. Displacement >5 mm is better treated surgically. |
| Lesser trochanter | Iliopsoas tendon | May cause LT or ischiofemoral impingement. Late excision or distal transfer for persistent pain. |
Greater Trochanter Avulsions
Displaced greater trochanter fractures in children appear to carry a high risk of avascular necrosis regardless of treatment method.