Symptomatic over coverage of the acetabulum can be treated well with resection of the rim of the acetabulum. Rim trimming certainly decreases impingement and increases FIR. Healthy FIR is 20–30 degrees. Every mm of rim resection gives 2–3 degrees increase of FIR.
Planning & Measurement
Acetabular wall coverage can be measured well on plain pelvis AP radiograph and the amount of resection can be planned. Intraoperatively, leaving the labrum attached to the articular cartilage while removing the bone allows measurement of the gap created against the 5.5 mm burr head. Trimming of more than 2–3 mm of bone is likely to make the labrum unstable requiring its repair. Bigger resections will do better with excision of the unsupported articular cartilage followed by labral repair.
Rim trimming may leave overhang of the bone above the resection that needs to be removed to prevent that bone from impinging on the femur. So, we extend the trimming till the anterior wall is flat all the way to the AIIS. This extent of resection does not leave any capsular attachment to the rim precluding capsular repair after rim trimming.
Resection Limits
Some papers suggest that 3mm of rim trimming is safe and 5mm leads to instability. Those authors do not seem to understand that 3 mm of bone is a lot to remove in a borderline dysplastic hip where as a patient with excessive coverage will not be unstable even with a 5 mm resection. The amount of rim resection should be based on the available extra bone and the required increase in FIR. Excessive rim resection can cause acetabular dysplasia and instability of the head.
Dr. Gourineni's Technique
Rim Trimming Approach
Goal is to get the right hip FIR to the healthy 20–30 range. Every mm of rim resection gives 2–3 degrees of FIR. So, a 7mm resection should give 15–20 degrees increase in internal rotation. Known dimensions of the burr and other instruments are used to measure the resection and bony and soft tissue landmarks to determine the location on the rim.
- Reflected head of rectus femoris attaches at 12 o'clock position of the acetabulum
- Iliopsoas tendon crosses at mid anterior point / 3 o'clock position
- The acetabular wall is thin at 12 and 3 becoming very thick between the 2 points with thickest part at AIIS level
- As the rim is resected the anterior wall appears as a triangle between 12, 3, and AIIS
Result
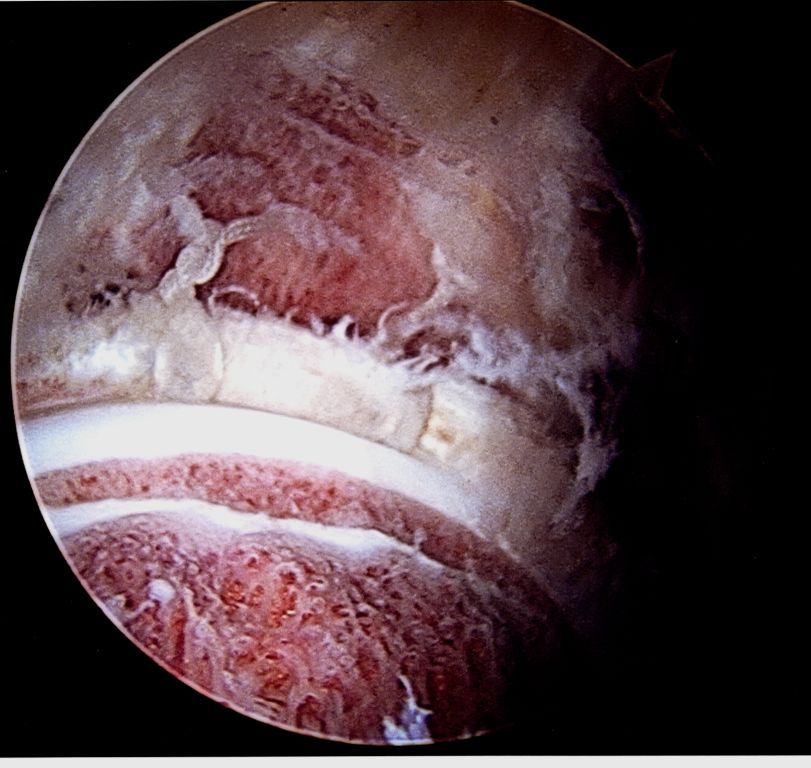
Arthroscopic image after acetabular rim trimming, labral repair with sutures, and femoral neck osteoplasty with open growth plate in the femoral head.