Key Fact
Hip capsule is 1 cm thick with the Iliofemoral ligament being the strongest ligament in the human body. Routine capsular repair restores anatomy and stabilizes the hip joint.
Open Hip Surgery
There are multiple ways to open the capsule with open surgery. 'T' and 'H' capsulotomy are common in open cases. 'Z' shaped capsulotomy is commonly used for safe surgical dislocation. Capsular repair is routine, but a tight repair can compromise femoral head circulation, especially after surgical dislocation and extended retinacular flap elevation. The capsule is left open or a small part excised after drainage of septic arthritis.
Hip Arthroscopy
Hip arthroscopy is difficult because of the joint's deep location, strong muscles, and a very thick capsule. Considerable force is required to penetrate the capsule with blunt instruments initially and it is not easy to find the initial hole for instrument exchange even with cannulas and switching sticks. Capsulotomy to enlarge the portal sites makes instrument passage easier.
| Capsulotomy Type | Description |
|---|---|
| Periportal | Enlargement of the portal sites — does not destabilize hip, but does not make extensive procedures easy |
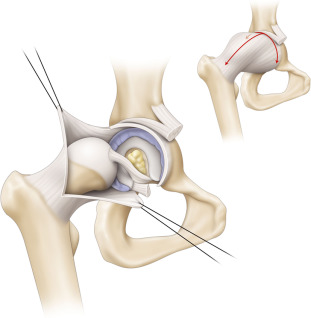
| Interportal | Releases the capsule parallel to the labral margin between two common portals from 12 to 3 o'clock — gives adequate exposure for acetabular work, but needs traction sutures to see more laterally on the neck |
| T-capsulotomy | Adds a longitudinal limb along the neck axis to the interportal capsulotomy — usually divides the Zona orbicularis along the fat plane between Iliocapsularis and Gluteus minimus muscles and shows the neck adequately |
| Capsulectomy | Limited fashion increases exposure, but precludes capsular repair |
Capsular Repair
Capsulorraphy seems to give better results compared to not repairing the capsule. Complete repair is shown to be better than partial repair. Both absorbable and non-absorbable sutures have been used successfully in various suture configurations. Some surgeons feel that disruption of the capsular repair is a common cause of postoperative pain and recommend repairing the capsule again or reconstructing the defect with thick dermal allograft.
Dr. Gourineni's Approach
Capsule Management in Practice
- Single portal for evaluating the cartilage in acetabular dysplasia
- Capsule repair selective in borderline dysplastics when not much rim trimming is done
- With adequate rim trimming, the medial attachment of the capsule to the acetabulum is disrupted and adequate repair is not feasible
- Most often medial capsulectomy when doing rim trimming — leaving nothing to repair
- Interportal capsulotomy is the routine approach